Shoulder Pain
Shoulder pain is an incredibly common condition, from young athletes, to the middle-aged and older population. As a student at Medical School, the shoulder was the “dreaded joint” that sent fear through us physiotherapy students. Little did I know that my first job as a newly qualified physiotherapist would see me working with an orthopedic surgeon, specializing in shoulder joint disfunction. I soon learnt not to fear the shoulder joint, but to respect it for it’s intricacies and complexity.

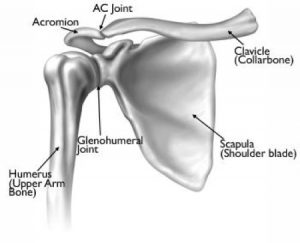
For the purposes of this discussion, I will focus on two of the articulations of the shoulder joint. The first is the gleno-humeral joint. This is a ball and socket joint, formed by the head of the humerus (the upper arm bone) and the glenoid fossa (socket) of the scapula. The surrounding ligaments, joint capsule, labrum, muscles and tendons are instrumental in providing stability to this joint. The second is the acromio-clavicular joint. It is this joint that is more often involved in cases of shoulder pain. This joint is at the very tip of the shoulder, above the gleno-humeral joint. It is formed by the acromion process of the scapula and the clavicle. Separating the acromio-clavicular joint from the gleno-humeral joint below, is the sub-acromial space. This space contains a bursa, the rotator cuff tendons and also the long head of the biceps tendon.
Your physiotherapist can often gain huge insight into the possible cause of your pain, just by taking a detailed history from you. A thorough assessment of the shoulder joint will often extend to assessment of the cervical spine, thoracic spine and general posture. Some things that may become evident on assessment are:
- restrictions in range of movement- an inability to fully lift the arm or to fully rotate the shoulder joint, very commonly the inability to reach the hand behind the back
- weakness of the muscles that stabilize the scapula- the bottom angle or even the entire medial border of the scapula may “wing” or lift off the rib cage
- poor posture- rounding of the thoracic spine or an increased forward head posture
- overactive neck or shoulder musculature that is compensating for weakness elsewhere, possibly the scapula stabilizers or the rotator cuff
- positive impingement signs- evidence of the rotator cuff or other tendons being compressed within the sub-acromial space
Assessment should be followed by patient education- a fundamentally important step to recovery. If a patient does not understand the underlying factors that contribute to their pain, then they cannot be expected to buy into the management or the rehabilitation thereof. Treatment will often include myofacial release of tight or over-active tissue, shoulder joint mobilization techniques, neural tissue mobilization, activation and strengthening of the scapula stabilizers or rotator cuff, postural correction, ergonomic advice for the most optimum workstation setup and a home exercise program. Of course, no two people are the same, and treatment must be tailored to the individual.
If you are experiencing shoulder pain, please do be assured that when approaching the shoulder joint, in a systematic way, with a thorough understanding of shoulder biomechanics, there is much that can be done to alleviate that pain.
Leave a Reply